Free DD 2870 PDF Form
In today's healthcare landscape, managing access to medical records can feel both complex and critical. Enter the DD 2870 form, a pivotal document for those within the military community. This form functions as a crucial tool for authorizing the disclosure of medical or dental information to specified individuals or entities. Whether it's needed to facilitate healthcare coordination, support claims for benefits, or assist in legal matters, the DD 2870 ensures that personal health information is shared securely and according to the patient's wishes. Understanding its parts, the process for completion, and its implications for privacy rights not only helps in navigating healthcare more effectively but also empowers individuals to take control of their personal health information. Its role might be specific, yet the DD 2870 form carries significant weight in ensuring that confidentiality is maintained, while also making sure that essential care and support are not hindered by bureaucratic barriers.
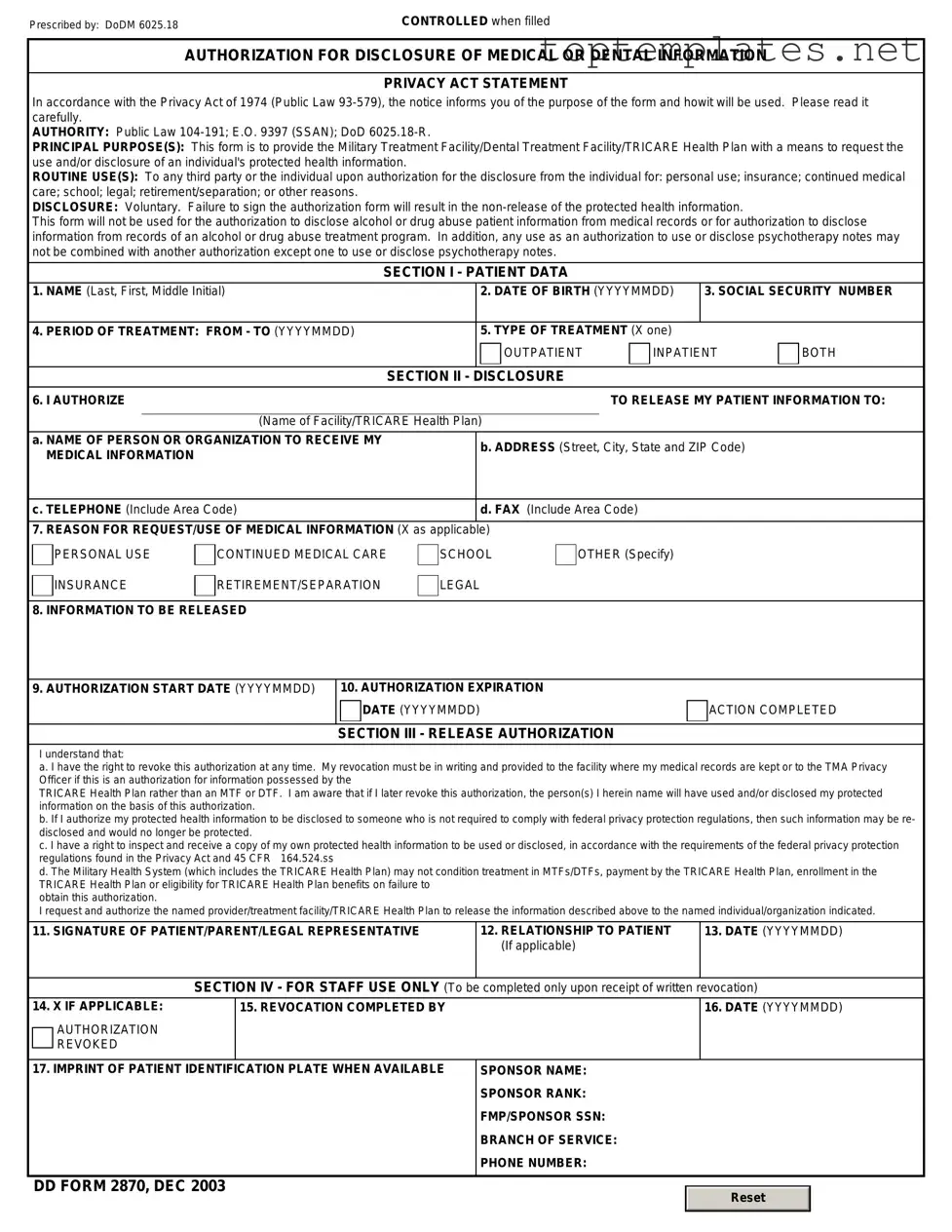
Sample - DD 2870 Form

Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
File Specs
| Fact Number | Description |
|---|---|
| 1 | The DD Form 2870, also known as the Authorization for Disclosure of Medical or Dental Information, is designed to allow individuals to request the release of their specific health information. |
| 2 | This form is used primarily within military health systems and by those who receive treatment at military medical facilities. |
| 3 | The information obtained through DD Form 2870 can be released to designated individuals, healthcare providers, or organizations as specified by the individual completing the form. |
| 4 | Completion of the DD Form 2870 is voluntary; however, not providing consent may limit the healthcare team's ability to share vital information with other healthcare providers or family members. |
| 5 | The form includes sections for identifying information about the individual whose records are being released, details of the information being requested, as well as the purpose of the disclosure. |
| 6 | To ensure privacy and protect personal health information, the DD Form 2870 includes a section for the expiration date of the authorization or a specific event after which the authorization is no longer valid. |
| 7 | Once completed and signed, the form should be submitted to the proper medical records department or healthcare provider holding the records. |
| 8 | The form aligns with the Health Insurance Portability and Accountability Act (HIPAA) guidelines to ensure that medical information is handled securely and confidentially. |
| 9 | There is no fee associated with submitting a DD Form 2870, but the process to obtain medical records may be subject to specific policies of the facility or organization. |
| 10 | While the DD Form 2870 is specifically for military or Department of Defense-affiliated individuals, civilian healthcare providers and institutions may have separate, similar forms in compliance with HIPAA for the release of medical information. |
Steps to Filling Out DD 2870
After deciding to request access to or the release of medical or dental records, it's necessary to complete the DD 2870 form accurately. This document serves as a permission slip, allowing designated individuals or entities to obtain the specified health information. Understanding and following the correct steps to fill out this form is crucial for a smooth process. Here’s a comprehensive guide to ensure the form is filled out correctly, promoting a swift and efficient handling of your request.
- Begin by gathering all necessary personal information, including full name, Social Security Number (SSN), date of birth, and contact details.
- On the form, start with Section 1. Fill out the patient's full name, including first, middle initial, and last name, along with their SSN or DoD identification number.
- In Section 2, provide the patient's date of birth using the mm/dd/yyyy format.
- Proceed to Section 3, where you should enter the patient’s full address. Include the street address, city, state, and ZIP code.
- For Section 4, specify the name of the military treatment facility (MTF) or the TRICARE Health Plan that currently holds the requested records.
- In Section 5, clearly indicate the purpose of the request by checking the appropriate box. If 'Other' is selected, provide a specific explanation.
- Section 6 requires the information of the individual or organization to whom the records will be released. Fill in the name, address, and, if applicable, the phone number.
- If the request includes a specification for dates of treatment or types of records needed, detail these in Section 7 and 8 respectively. Be as clear and concise as possible.
- In Section 9, the requester must sign and date the form, legally authorizing the release of the specified information.
- Lastly, review the completed form for accuracy and completeness. Any missing or incorrect information can delay the process.
Once the DD 2870 form is fully completed and checked for accuracy, it must be submitted to the appropriate office as indicated by the instructions specific to the facility or health plan. Timely and correct completion of this form is key to facilitating the desired access or release of medical records without undue delay.
Discover More on DD 2870
What is the DD 2870 form used for?
The DD 2870 form, also known as the Authorization for Disclosure of Medical or Dental Information, serves a critical function in allowing military members, their families, and other authorized individuals to grant permission for the release of their medical or dental records. This form facilitates the process of sharing pertinent health information with specified individuals or entities, ensuring that the disclosure complies with privacy laws and regulations.
Who should fill out the DD 2870 form?
Individuals who wish to authorize the disclosure of their medical or dental records, or those of their dependents, should complete the DD 2870 form. This includes active duty military personnel, retirees, and their authorized family members. It's also applicable to anyone who has received medical or dental care through a military facility or program and now requires the release of those records to a third party.
What information is needed to complete the DD 2870 form?
To accurately fill out the DD 2870 form, individuals will need to provide detailed information, including the patient's full name, Social Security Number (SSN), and date of birth. The form also requires the specifics of the information being requested, such as the type of records or the dates of service to be disclosed. Additionally, the recipient's name and address, the purpose of the disclosure, and any expiration date for the authorization must be clearly stated. The requester's signature and date complete the authorization process.
How does one submit the DD 2870 form after completing it?
After filling out the DD 2870 form, it should be submitted to the appropriate military medical or dental facility where the records are held. The contact information and submission process may vary between facilities, so it is advisable to contact the specific facility directly to verify the correct submission procedure. This may involve mailing the form, electronic submission, or delivering it in person, depending on the facility's policies.
Is there an expiration date for the DD 2870 form?
Yes, individuals can specify an expiration date for the authorization on the DD 2870 form. If no date is provided, the authorization will typically remain in effect for one year from the date of the signing. Specifying an expiration date ensures that the authorization for release of medical or dental information is limited to the time frame intended by the requester.
Can the DD 2870 form be revoked?
Indeed, the authorization granted by completing the DD 2870 form can be revoked at any time by the individual who initiated it. To revoke the authorization, written notice must be delivered to the medical or dental facility that holds the records. It's important to note that the revocation will not affect any previously allowed disclosures of information made in reliance on the original authorization before the revocation was received and processed.
Common mistakes
When filling out the DD 2870 form, which is used to authorize disclosure of medical or dental information, people often make mistakes that can lead to delays or denials in processing. Being aware of these common errors can help ensure the process is smooth and successful.
-
Not verifying eligibility - Before completing the form, individuals fail to confirm their eligibility for the release of the requested medical information. This step is essential to prevent rejection of the request.
-
Incomplete patient information - Leaving blank fields in the patient section or providing incomplete information can result in processing delays. Full name, date of birth, and other relevant identification details must be accurately filled in.
-
Lack of specificity - Often, people do not specify the type of records needed, such as medical history, lab results, or specific dates of service. This lack of detail can lead to an incomplete information release.
-
Incorrect authorization details - The section that requires designation of authorized individuals or entities is frequently filled out incorrectly. Clear identification of who is authorized to receive the information is crucial.
-
Forgetting to sign and date - A common oversight is neglecting to sign and date the form. An unsigned or undated form is considered invalid and will not be processed.
-
Not stating the purpose of the request - Failing to declare the purpose for the information request can lead to unnecessary scrutiny or processing delays. Whether it is for personal use, insurance purposes, or continuing medical care, the intent must be clear.
-
Improperly requested time frame - Individuals may inaccurately specify the time frame for which they need the records, either requesting too broad a period or an incorrect range, thereby complicating record retrieval.
-
Misunderstanding HIPAA regulations - A limited understanding of Health Insurance Portability and Accountability Act (HIPAA) regulations can lead to confusion about what information can be legally disclosed and under what circumstances.
-
Use of incorrect form version - Using an outdated version of the DD 2870 form can result in denial of the request, as current guidelines and privacy acts may not be addressed.
-
Failure to specify distribution method - People often omit how they wish to receive the information, such as by mail, fax, or electronic means. Specifying the preferred distribution method can expedite the process.
By paying attention to these common mistakes and taking care to fill out the DD 2870 form accurately and thoroughly, the process of requesting and receiving medical or dental records can be made more efficient and effective.
Documents used along the form
When navigating through the healthcare system, especially within the military or government services, a variety of forms and documents are often required to authorize, request, or obtain medical records or services. The DD 2870 form is one such document widely recognized for authorizing disclosure of medical or dental information. However, it's rarely the only document needed. Alongside the DD 2870, several other forms and documents play pivotal roles, depending on the situation. Here’s a succinct look into ten additional forms and documents that are frequently used in conjunction with the DD 2870.
- Standard Form 180 (SF-180) - Primarily used to request military service records, it's essential for verifying service for benefits, retirement, employment, and membership in veterans' organizations.
- Health Insurance Portability and Accountability Act (HIPAA) Authorization Form - This document allows healthcare providers to disclose the individual's health information to third parties, complying with privacy regulations.
- DD Form 214 - The Certificate of Release or Discharge from Active Duty is critical for veterans, serving as evidence of military service and qualifications for benefits.
- DA Form 31 - Used by Army personnel to request and authorize leave from duty; often needed alongside medical records for processing medical leaves or related benefits.
- VA Form 10-10EZ - Application for Health Benefits, this form is used by veterans to apply for medical benefits through the Department of Veterans Affairs.
- Consent for Treatment Form - A generic form allowing healthcare practitioners to perform medical procedures or treatments, often necessary in conjunction with medical record requests.
- Privacy Act Request Form - Used to request personal records under the Privacy Act, it complements the DD 2870 when accessing personal health or service records.
- Medical Records Release Form - Similar to the DD 2870, this form might be used in non-military healthcare contexts to authorize the release of medical records to third parties.
- Claim for Disability Compensation and Related Compensation Benefits (VA Form 21-526EZ) - Veterans use this form to claim disability benefits, often requiring accompanying medical records.
- Appointment of Veteran’s Service Organization as Claimant’s Representative (VA Form 21-22) - Authorizes a service organization to act on behalf of veterans in preparing, presenting, and prosecuting claims for benefits. This is crucial for veterans needing assistance with their claims and often accompanies requests for medical records.
Understanding and utilizing these forms correctly is vital for efficiently navigating healthcare and benefit systems, especially within the context of military and veterans' affairs. While the DD 2870 may begin the process of accessing needed information, these accompanying documents ensure that all aspects of healthcare, benefits, and service verification are covered comprehensively. Whether you're a service member, veteran, or supporting a family member in these areas, being acquainted with these forms will streamline processes and enhance access to deserved benefits and services.
Similar forms
- Health Insurance Portability and Accountability Act (HIPAA) Authorization Form:
Similar to the DD 2870 form, the HIPAA Authorization Form permits the release and sharing of an individual's health information. Where the DD 2870 is geared towards military personnel, the HIPAA form applies broadly to all patients wishing to allow health care providers to disclose their personal health information to specified parties.
- Power of Attorney (POA) for Health Care:
This document enables individuals to designate someone else to make health care decisions on their behalf, should they become unable to do so. Like the DD 2870, it focuses on decisions about the individual’s health care and personal welfare, including access to medical records.
- Family Educational Rights and Privacy Act (FERPA) Release Form:
FERPA Release Forms allow disclosure of a student's educational records to third parties, similar to how the DD 2870 allows for the sharing of medical records. While FERPA pertains to educational information, both forms serve the function of granting permissions for the release of personal information.
- Form 8822 by IRS:
This form is used for changing the address with the Internal Revenue Service. Despite focusing on a different type of information (tax information versus medical records), both Form 8822 and the DD 2870 involve the process of updating personal information and notifying respective authorities for the continued accuracy of records.
- Consent for Release of Information (Social Security Administration):
Similar to the DD 2870, this consent form allows the Social Security Administration to release personal Social Security information to designated individuals or organizations. Both forms are vital in managing and safeguarding personal information, albeit for different purposes.
- Medical Release Form for Minors:
Often used by schools or sports organizations, this form permits the sharing of a minor's medical information with specified parties, typically in emergency situations. Like the DD 2870, it is focused on healthcare information but tailored specifically towards the needs and protection of minors.
- Employment Verification Form:
While primarily used for verifying employment status, this form shares a similarity with the DD 2870 in that it involves the process of sharing specific personal information (in this case, related to employment) with authorized parties based on the individual's consent.
Dos and Don'ts
Filling out the DD 2870 Authorization for Disclosure of Medical or Dental Information form requires careful attention to ensure accurate and proper use. To help guide you through this process, here are eight key dos and don'ts:
- Do carefully read all the instructions before beginning to fill out the form to ensure you understand each section's requirements.
- Don't rush through the form without verifying all the information you provide is current and accurate. Mistakes can delay processing.
- Do use black ink or type directly into a digital form if available. This makes the form easier to read for processing.
- Don't leave any required fields blank. If a section does not apply, fill it with "N/A" (not applicable) to indicate you didn’t overlook it.
- Do include your signature and the date in the designated areas. Your form cannot be processed without this verification.
- Don't forget to specify the purpose of the request by clearly stating why you need the medical or dental information and how it will be used.
- Do review the authorization section to understand which records will be disclosed and ensure you're comfortable with the terms before signing.
- Don't disregard the expiration date of your authorization. Remember, your consent to release records is not indefinite and will require renewal.
Misconceptions
The DD 2870 form, known as the Authorization for Disclosure of Medical or Dental Information, plays a vital role in managing the privacy and accessibility of healthcare records for military personnel and their families. However, several misconceptions surround its use and implications. Correcting these misunderstandings is crucial to ensure that individuals are well-informed about their privacy rights and how they can exercise them properly.
Misconception 1: The DD 2870 form grants unlimited access to one's medical records. Many believe that once signed, the DD 2870 form provides the requester with unrestricted access to the individual's entire medical history. This is not accurate. The form allows for the specification of what information can be disclosed and for what purpose, offering a way to limit access to only relevant information.
Misconception 2: Only military personnel can use the DD 2870 form. While it's commonly associated with service members, the form is also available for their dependents. This means spouses and children who are eligible for military healthcare benefits can also authorize the release of their medical or dental information when necessary.
Misconception 3: Once signed, the authorization is permanent. Some assume that after signing the DD 2870 form, the authorization remains in effect indefinitely. In truth, the form allows the individual to set an expiration date for the authorization, ensuring control over the duration of the granted access.
Misconception 4: Electronic signatures are not allowed on the DD 2870 form. With the growing reliance on digital processes, there's a belief that the DD 2870 must be printed and signed physically. However, in many cases, digital signatures are accepted, facilitating easier submission and faster processing times. This policy can vary by facility, so it's advisable to check with the specific medical facility handling the request.
Understanding the DD 2870 form and its actual applications helps service members and their families navigate their healthcare privacy rights more effectively. Dispelling these myths ensures individuals make informed decisions regarding the disclosure of their medical or dental information.
Key takeaways
When addressing the process of filling out and using the DD 2870 form, which is the Authorization for Disclosure of Medical or Dental Information, it's critical to grasp the numerous facets that govern how this form is handled. This document plays a crucial role in the authorization and restriction of personal health information disclosure. Here are key takeaways to guide individuals in managing this crucial document effectively:
- Understanding the Purpose: The DD 2870 form is designed to authorize the release of medical or dental records. It's used by military personnel, their dependents, and civilians receiving care through military health services.
- Know the Information Required: Completing the form requires detailed personal information, including the full name, Social Security Number (SSN), or Department of Defense (DoD) identification number, and the specific information being requested for disclosure.
- Specifying Information to be Disclosed: The form allows individuals to specify which parts of their medical record they consent to disclose. This could range from a comprehensive medical record to specific documents like lab reports or imaging studies.
- Stating the Purpose of Disclosure: Clearly indicating the reason for the request is mandatory. Purposes can include personal use, insurance claims, continuing medical care, or legal matters.
- Designating the Recipient: The individual completing the form must identify the organization or individual who is authorized to receive the medical or dental information. This ensures that the data is shared only with the intended party.
- Limited Time Frame: Authorization granted by the DD 2870 is typically valid for a limited period, usually not exceeding one year. It's important to note the specific expiration date on the form.
- Right to Revoke Permission: The form allows individuals to withdraw their consent for the disclosure of their medical information at any time. This revocation must be submitted in writing.
- Signatures are Mandatory: For the authorization to be valid, the form must be signed by the individual whose records are being released or by a legal representative if the individual is incapable of signing.
- Privacy and Security: The DD 2870 form ensures that personal health information is shared in compliance with privacy laws, protecting the individual’s confidentiality and security.
- Understanding State Laws: While the DD 2870 form is a federal document, it's important to be aware of any state-specific regulations that might affect the disclosure of medical records.
In conclusion, the DD 2870 form is a vital tool for managing the disclosure of personal medical and dental information within the framework of military health services. Proper completion and understanding of the form's elements ensure that individuals can securely and efficiently manage the sharing of their health information according to their wishes, while respecting legal requirements and personal privacy.
Common PDF Forms
Lease to Own Trucking Companies - Prohibits the owner operator from displaying the carrier's name on their vehicles without prior written consent, protecting the carrier's brand.
Da 638 - A key form in the Army’s recognition program, ensuring deserving individuals are honored for their contributions.
Puppy Health Record - Easily communicate your puppy's health history and care needs with veterinarians and caregivers, making transitions and visits smoother.